


Re-Understanding Diabetes
Part 2: The Fat Insulin Resistance

In the first part of this series, we revisited our understanding on what diabetes is and how it occurs in the body. If you missed it, you can read it here:
Re-understanding Diabetes

What if I told you that what most people believe about diabetes is actually not 100% true?
It is important to note that insulin resistance cannot be seen from the outside—it is a condition that reflects the internal state of your body; specifically your liver, muscles, adipose tissue, pancreas, and blood vessels.
While type 2 diabetes is caused by insulin resistance, and type 1 and 1.5 diabetes result from an autoimmune reaction, the diet-induced insulin resistance present in both conditions is biologically identical. In fact, a growing body of scientific evidence demonstrates that insulin resistance is a growing concern in autoimmune diabetes owing to less-than-ideal lifestyle choices and eating a diet that mainly consists of low-carbohydrate foods like meat, fish, dairy, eggs, and oils, or a diet containing significant quantities of refined sugar and processed foods (1,2).
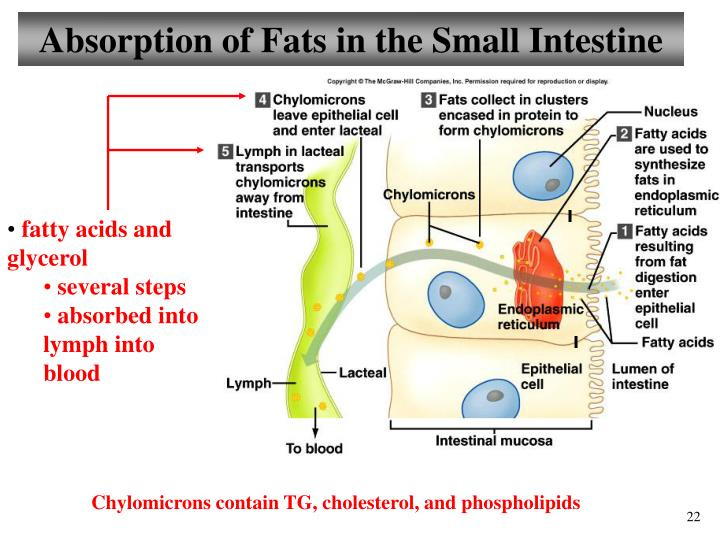
When you eat foods containing fat-soluble nutrients (including triglycerides, phospholipids, and cholesterol), two important processes occur in your small intestine. First, the cells in the lining of your small intestine absorb these fat-soluble nutrients and package them into particles called chylomicrons, which are then dumped into your lymphatic system. When the lymphatic fluid ushers’ chylomicrons into your blood, they’re circulated throughout your body so that your adipose (fat) tissue and muscle have the first chance to uptake the triglycerides from your food.
When your small intestine detects fat-soluble nutrients in your food, it releases a collection of powerful hormones that communicate with your brain and stomach to control your appetite and slow your gastric emptying rate. Your small intestine then signals your stomach to slow down the digestion process. This is because the fatty meal is going to take some time to fully digest and absorb the nutrients. A slowed gastric emptying rate results in an upstream traffic jam, slowing down the passage of chyme out of your stomach and into your small intestine. This effect is one reason why diets high in fat are effective at curbing your appetite and making you feel full for long periods of time.
As a result of the simultaneous fat absorption into your lymphatic system and slowed gastric emptying rate, both carbohydrate and protein digestion are slowed. The consequence is that fat-rich chylomicrons appear in your blood more rapidly than glucose (one of the building-blocks of carbohydrates) and amino acids (the building blocks of protein). When fat-rich chylomicron particles have circulated throughout your body and have off-loaded triglycerides, your liver then uptakes the remaining particles.
The triglyceride molecules are then transferred into lipoprotein particles and sent out in your blood once again. With the help of enzymes located on the surface of cells throughout your body, tissues absorb fatty acids and cholesterol from these lipoproteins. Unlike glucose, fatty acids can enter cells easily without requiring an escort like insulin. It is good to note that while insulin can certainly help fatty acids get out of lipoproteins and into tissues, insulin is not fully required since fatty acids can also enter tissues without insulin. Because of this, tissues have no choice but to absorb fatty acids when they appear in your blood in large amounts.
As soon as the fatty acids are absorbed by cells in your liver and muscle tissues, they are either burned for energy or stored for later use. Those that are burned for energy are immediately ripped apart and transported to the mitochondria to be turned into ATP (the cellular equivalent of energy), and those that are stored enter a pool of fatty acids inside the cell, known as a “lipid droplet”.
Unlike other tissues with a distinct location in your body such as your brain, heart, or lungs, your adipose (fat) tissue is located in many places. You can find small and large pockets of fat almost everywhere, in the abdomen, butt, thighs, lower back, chest, armpits, face, neck, and even ankles. Fatty acids enter your adipose tissue in the exact same way that they enter all other tissues—aided by enzymes known as lipases and fatty acid transport proteins (FATPs). Fatty acids are easily absorbed because your adipose tissue contains the perfect molecular machinery to uptake and store fatty acids for long periods of time. In fact, that’s exactly what your adipose tissue is designed to do.
While most people want to minimize the amount of adipose tissue on their body, it’s important to point out that adipose tissue is actually a protective organ. Your adipose tissue is designed to grow and shrink in response to times of feast and times of famine- storing energy at times when there are excess calories available to protect you for when calories are sparse. However, if one tends to store more fat in their abdomen, the higher the risk for obesity, cardiovascular disease, hypertension, diabetes, and insulin resistance (it’s all about balance and understanding what YOUR body needs).
The biology of adipose tissue insulin resistance is fascinating and deserves an explanation. To start, fat cells are incredibly flexible and are designed to store large quantities of fat, but they cannot expand indefinitely. Chronically overfed fat cells become inflamed just like other tissues can, and as a result, the low-grade chronic inflammation triggers insulin resistance.
Over time, cells in your adipose tissue can burst open, spilling their contents into the interstitial fluid that surrounds the tissue. This explosion releases cellular debris into your blood and causes neighboring cells to release stress signals called “Cytokines” (a term heard a lot during covid), into your blood. This then recruits cells called “Macrophages” to invade the tissue in search of unwanted cellular debris from ruptured cells. When the cellular debris becomes too much for Macrophages, they recruit more Cytokines, creating more Macrophages- the issue though is that this process does not just recruit more Macrophages, it triggers chronic inflammation and creates a state of adipose tissue insulin resistance.
Even though your muscles and liver can generate ATP from glucose, fatty acids, and amino acids, your muscles and liver are designed to use glucose as their primary fuel. Since fatty acids appear before glucose during the digestion process, your muscles and liver are exposed to more fatty acids than glucose, setting the stage for insulin resistance when glucose becomes more readily available. When your muscles and liver uptake fatty acids from your blood, they also upregulate enzymes involved in all aspects of fatty acid metabolism and downregulate enzymes involved in all aspects of glucose metabolism—because fatty acids are now the predominant fuel. When cells in your liver and muscles begin burning and storing fatty acids- just as Philip Randle described, they block glucose from entering because the cellular machinery required to uptake, process, and store glucose has been deprioritized.
As a result of this process, cells in your liver and muscle alter their internal enzymatic machinery based on the fuel that is most readily available. So, when you check your blood sugar level two to six hours after eating a meal containing predominantly fat and protein, you may see a high number and wonder why. This is exactly when insulin rejection first takes place. Unlike your adipose (fat) tissue, which is specifically designed to store fat to protect other organs from fat overload, your muscle and liver tissues are designed to store small amounts of fat and large amounts of glycogen. But when your liver and muscles first absorb fat from your blood following a fat-rich meal, they respond by rejecting insulin to block glucose from entering, because they have already accepted fatty acids as their primary energy source. First come, first served!
One of the most common side-effects of eating a high-fat diet is fatty liver disease (also known as non-alcoholic fatty liver disease or NAFLD). Fatty liver disease occurs when the amount of fat in your liver is more than 5 percent by weight, resulting in liver enlargement, which can then lead to liver fibrosis. While it’s true that eating or drinking refined sugars like sucrose and high-fructose corn syrup (HFCS) can contribute to fatty liver disease, a growing body of research shows that a high-fat diet results in a progressive decline in liver function over time (3, 4, 5).
Your liver is a crucial part of the insulin resistance equation because cells in your liver are capable of exporting glucose into your blood to provide your brain with a constant supply of glucose at all times. Insulin is the signal that tells your liver exactly when to increase and when to decrease the amount of glucose it exports. Herein lies the problem: When you develop insulin resistance in your liver due to the accumulation of excess dietary fat, your liver can’t communicate with insulin very effectively, resulting in a chronically high rate of glucose export, high fasting blood glucose, and high post-meal blood glucose. The effect: an accumulation of excess fatty acids prevents your liver from accurately controlling how much glucose it releases into your blood.
So, what is the link between diabetes and cancer? First, we need to understand that thanks to epigenetics, we know that genetics actually have very little to do with the expression of dis-ease in the body, like cancer and diabetes (just to name a couple). Epigenetics has taught us that the expression of genes is changeable. We will go further into the diabetes-cancer connection in the next part of this series.

Resources
Insulin Resistance: From Mechanisms to Therapeutic Strategies - PMC (nih.gov)
Mechanisms and disease consequences of nonalcoholic fatty liver disease: Cell
Additional Readings of Interest: